

January QMNC Research Roundup
This month, QMNC members’ research invites reflection on who holds power in maternity care, whose knowledge counts, and how systems can better support physiologic, respectful birth. Members shared research that explores midwifery education, delivery models, monitoring practices, home birth, tools, and equity to show how structures and social identities shape experiences and outcomes.
Dive in and explore the January Research Roundup!
Midwifing Medical Education and Residency Training
How midwives can transform medical education
 This award-winning poster by Christy Santoro (Honourable Mention, 2025 ILBRC), explores the potential of incorporating midwives into undergraduate and graduate medical education. They outline how midwives can foster cultural change in medical training, promoting physiologic birth and reducing unnecessary interventions. Emerging praxis includes advancing a demedicalized foundation for pregnancy and birth, integrating reproductive justice, using narrative and embodied learning tools, and advocating for recognition of diverse ways of knowing. Intervening early in medical education is key to early influence of factors that shape over-medicalized views of birth, countering myths about midwifery, and reshaping reproductive care narratives. Creating pathways for midwives in medical training could help build a future workforce grounded in interprofessional collaboration and respectful, humanistic care across settings.
This award-winning poster by Christy Santoro (Honourable Mention, 2025 ILBRC), explores the potential of incorporating midwives into undergraduate and graduate medical education. They outline how midwives can foster cultural change in medical training, promoting physiologic birth and reducing unnecessary interventions. Emerging praxis includes advancing a demedicalized foundation for pregnancy and birth, integrating reproductive justice, using narrative and embodied learning tools, and advocating for recognition of diverse ways of knowing. Intervening early in medical education is key to early influence of factors that shape over-medicalized views of birth, countering myths about midwifery, and reshaping reproductive care narratives. Creating pathways for midwives in medical training could help build a future workforce grounded in interprofessional collaboration and respectful, humanistic care across settings.
See the poster and join the conversation here.
Fetal Monitoring and Physiologic Birth
How continuous electronic fetal monitoring shapes women’s experiences
In this systemic integrative review, Sarah Murray, Deborah J. Fox, Rebecca L. Coddington, Vanessa L. Scarf, examine how continuous electronic fetal monitoring (CEFM) shapes women’s labour experiences across high-income countries. Eighteen studies were categorized into three themes: “Feeling reassured versus anxious about the welfare of their baby,” “Feeling comfortable and free to be mobile versus feeling uncomfortable and restricted,” and “Feeling respected and empowered to make decisions versus feeling depersonalised with minimal control." Findings indicate that CEFM often restricts mobility, increases anxiety, and contributes depersonalized care. The authors recommend designing and implementing monitoring technologies that maximize freedom of movement, comfort, and increase the sense of control and choice for women.
Continue the discussion here.
Respectful Maternity Care and Intersectionality in LMICs
Social identities shape care experiences
This systematic review of 17 studies across 15 low- and middle-income countries by Victor Abiola Adepoju, Chioma Odueniyi, Abdulrakib Abdulrahim, Qorinah Estiningtyas Sakilah Adnani explores how intersecting factors such as age, poverty, ethnicity, disability, marital status, and migration, shape women’s experiences of respectful maternity care. The authors find that women who are young, poor, unmarried, less educated, and from certain ethnic or caste groups, migrants, or those living with disabilities are disproportionately exposed to neglect, verbal abuse, non-consented procedures and exclusion from decision-making. They identify three key mechanisms driving inequities: social stigma and moral judgement, provider bias about who is “deserving” of care, and communication barriers, including literacy and language. They find these barriers are systemic, structural inequities. They present a conceptual model offering a explanatory framework:
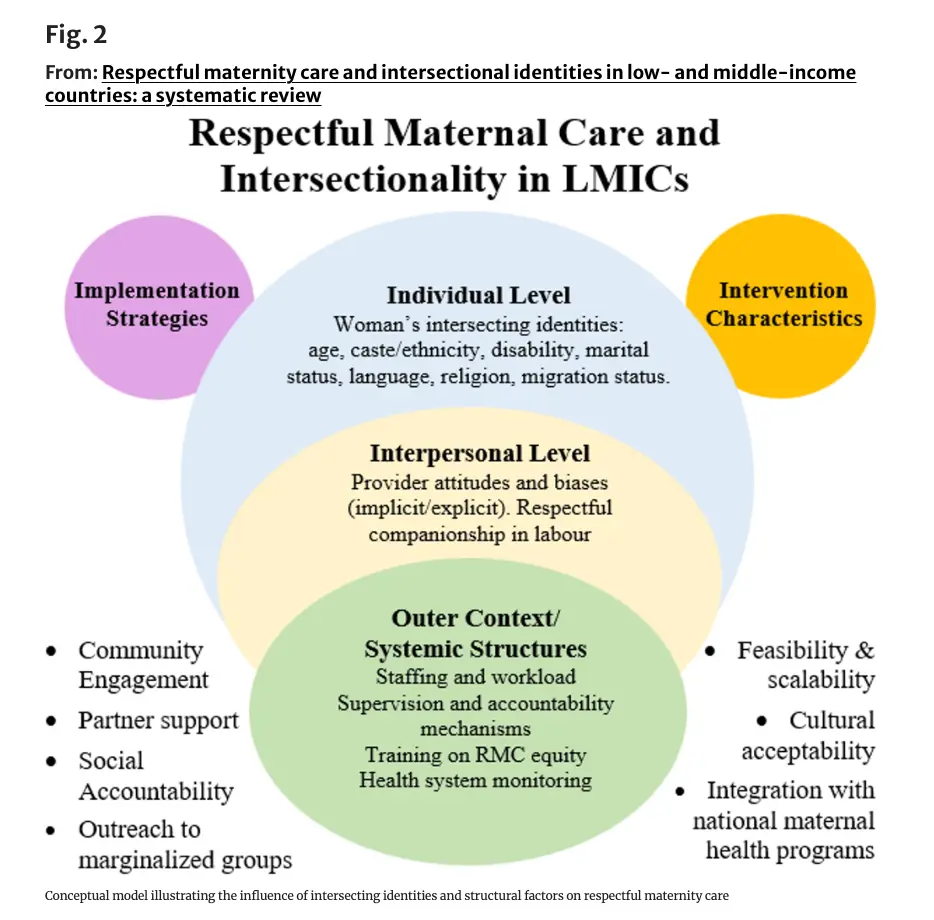
Fig 2… “illustrates how individual identity axes (such as caste, disability, age, migration status or literacy) interact with structural drivers such as provider biases, resource constraints, and facility norms, in shaping respectful or disrespectful care. By mapping these interactions, the model underscores that vulnerabilities are multiplicative vis-a-vis layered identities intensify exposure to stigmatization, neglect, and abuse. It also identifies leverage points for intervention, including anti‑bias training, community oversight, inclusive infrastructure and accountability mechanisms. Thus, the model translates intersectional theory into actionable strategies for improving respectful maternity care.”
Continued the discussion here
Obstetric Violence in Uruguay
Legal recognition vs practice gaps
Romina Gallardo, one of the authors of an article in Humanising Birth, which was featured in the November Research Roundup, has shared two related Spanish-language papers on obstetric violence in Uruguay. She offers this summary of the most recent article which “analyzes how obstetric violence is conceptualized in Uruguay and the difficulties in applying it in legal practice, highlighting the tensions between the legal framework, medical practice, and feminist struggles. The paper argues that the legal recognition of obstetric vio-lence in Uruguay is a symbolic but insufficient advanced. Conceptual problems, regulatory gaps, and institutional resistance persist, limiting the effective protection of the rights of women and pregnant people. To overcome these challenges, the authors propose rethinking the notion of autonomy from a feminist, intersectional, and relational perspective, incorporating theoretical contributions on epistemic injustice, and implementing effective mechanisms for prevention, reporting, and punishment.”
See both of Romina’s articles here
Home Birth: LMIC and HIC perspectives
Through the lens of “too little to late” and “too much too soon.”  Ruth Terry and Farzeneh Pazandean examined global and local trends in home birth through the lens of “too little to late” and “too much too soon.” They found in low-resource settings, home birth without support can contribute to poor outcomes, while in high-income countries, over-medication of hospital births is a contributor to suboptimal. They emphasize that home birth is recognized as a human right in many European countries and can support physiologic, low-intervention care for low-risk families. Ruth has launched a new special interest group on Home Birth Research and invites those that are interested to join the group and continue the discussion here
Ruth Terry and Farzeneh Pazandean examined global and local trends in home birth through the lens of “too little to late” and “too much too soon.” They found in low-resource settings, home birth without support can contribute to poor outcomes, while in high-income countries, over-medication of hospital births is a contributor to suboptimal. They emphasize that home birth is recognized as a human right in many European countries and can support physiologic, low-intervention care for low-risk families. Ruth has launched a new special interest group on Home Birth Research and invites those that are interested to join the group and continue the discussion here
Factors Influencing and Monitoring Home Births in LMICs
Also exploring home birth, these slides were shared at presentation at the International Labour and Birth Research Conference symposium “QMNC: Measuring Quality of Care,” and are now available to our community. They describe a scoping review by QMNC Fellows Amir Ali Samnani, Lorena Ibarguen, along with QMNC co-leads Allison Cummins and Melissa Cheyney, to map and summarize existing evidence on the factors influencing home births and the community-based platforms that support and monitor them in low and middle income countries. Preliminary findings highlight the role of cultural norms, family and community support, and relationships with healthcare providers in influencing care-seeking. Traditional birth attendants and community health workers play key roles in supporting safer home births.
View the slides and continue the discussion here
QMNC Priority 3 project advances
Review of Metrics and Tools for Evaluating Care Within The QMNC Framework’s Philosophy Component, and Developing the QMNC Tool Registry

Slides are also available now for the QMNC Measuring Quality of Care symposium on research projects underway for Priority 3. The work of QMNC Fellows Florence Darling along with Qorinah Adnani, Melissa Cheyney and Saraswathi Vedam was presented on evaluating of metrics and tools for the QMNC Framework’s Philosophy component, and development of a registry of metrics and tools to support QMNC’s research priorities.
View the slides and continue the discussion here.
Thank you to everyone who shared their work and reflections this month. This collection illustrates the many ways researchers, clinicians, and communities are contributing to improved maternal and newborn care. Does this research resonate with your work or experience? Join the conversation by commenting below or engaging directly with the original posts shared by members of the QMNC Research Alliance.